Article Text

Abstract
Objective To determine the effectiveness of physical activity interventions involving mobile applications (apps) or trackers with automated and continuous self-monitoring and feedback.
Design Systematic review and meta-analysis.
Data sources PubMed and seven additional databases, from 2007 to 2020.
Study selection Randomised controlled trials in adults (18–65 years old) without chronic illness, testing a mobile app or an activity tracker, with any comparison, where the main outcome was a physical activity measure. Independent screening was conducted.
Data extraction and synthesis We conducted random effects meta-analysis and all effect sizes were transformed into standardised difference in means (SDM). We conducted exploratory metaregression with continuous and discrete moderators identified as statistically significant in subgroup analyses.
Main outcome measures Physical activity: daily step counts, min/week of moderate-to-vigorous physical activity, weekly days exercised, min/week of total physical activity, metabolic equivalents.
Results Thirty-five studies met inclusion criteria and 28 were included in the meta-analysis (n=7454 participants, 28% women). The meta-analysis showed a small-to-moderate positive effect on physical activity measures (SDM 0.350, 95% CI 0.236 to 0.465, I2=69%, T 2=0.051) corresponding to 1850 steps per day (95% CI 1247 to 2457). Interventions including text-messaging and personalisation features were significantly more effective in subgroup analyses and metaregression.
Conclusion Interventions using apps or trackers seem to be effective in promoting physical activity. Longer studies are needed to assess the impact of different intervention components on long-term engagement and effectiveness.
- physical activity
- app
- accelerometer
- behaviour
- effectiveness
Statistics from Altmetric.com
Introduction
Physical activity is essential to the prevention and treatment of multiple chronic conditions1 2 and can prevent premature mortality.3 Any intensity of physical activity substantially reduces risk of death in a dose–response manner.4 Nonetheless, more than a quarter of adults worldwide are insufficiently active,5 and physical inactivity represents a leading cause of death worldwide.6 The global pandemic of physical inactivity is responsible for at least $67.5 billion of economic burden per year.7
Behaviour change interventions to promote physical activity can include several behaviour change strategies and components—so-called behaviour change techniques (BCTs).8 Two BCTs seem to be particularly effective: self-monitoring and feedback on behaviour.9 For instance, interventions using pedometers can facilitate self-monitoring and feedback on step counts, having shown significant improvements in the short term (4 months).10 11 However, these pedometer interventions are burdensome to maintain, as users have to use a step diary to keep track of their step counts.
In contrast, modern-day smartphone applications (apps) and activity trackers (eg, wearable fitness bands and smartwatches) enable automated and continuous self-monitoring and feedback on physical activity. Current smartphones and trackers enable the burdenless measurement of activity with acceptable accuracy,12 as well as allow for continuous access to recorded data (longitudinally and in real time), via apps or the tracker’s display. Nevertheless, a major challenge with apps and trackers is their high drop-off rate,13 with reports of a third of users of activity trackers abandoning their device in the first 6 months.14 It has been suggested that reducing user burden and providing features like goal setting, personalisation and game-like functionality (ie, gamification) may facilitate engagement, promote retention and increase intervention effectiveness.15–17
Existing reviews of apps and trackers have not yet focused on seemingly healthy adults18–23 and technology enabling automated and continuous self-monitoring and feedback, with apps often still requiring users to connect an accelerometer to a computer periodically via a hardware connection.20 22 24–30 These reviews of older apps and trackers have shown non-significant22 24 26 or small-to-moderate positive results20 25 28 with high heterogeneity, often mixing very different types of populations apart from healthy adults (eg, children,26 elderly22 27 28 and chronic conditions20 25 27 28). Furthermore, retention and engagement with these interventions, and effectiveness of different intervention features (eg, personalisation and gamification) have seldom been analysed.
The aim of this systematic review and meta-analysis was to evaluate the characteristics and effectiveness of interventions involving contemporary mobile apps or physical activity trackers (ie, enabling automated and continuous self-monitoring and feedback) in promoting physical activity, as well as in improving engagement and retention, in adults (18–65 years old) without chronic disease. A secondary aim was to explore and compare the effect of specific features in these interventions using metaregression.
Methods
This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.31 We followed a protocol registered with PROSPERO (CRD42017057854) for a broader review on physical activity, diet and weight loss. This paper focuses on physical activity; papers focusing on weight loss and diet were excluded at the full-text screening stage and will be analysed in a separate publication.
Search strategy
A search of the literature was performed in January 2017 (and updated continuously up to January 2020) using PubMed, Embase, CINAHL, PsycInfo, SciELO, ACM Digital Library, Cochrane Central Register of Controlled Trials and ClinicalTrials.gov. Articles were included if published between January 2007 and January 2020 since the launch of the first app stores. No language restrictions were applied. Search strings combined free terms (eg, smartphone, application and wearable) and controlled vocabulary (complete search strategy in online supplemental eMethods). Reference lists of relevant articles were also screened. Citations were uploaded to EndNote V.X9, where duplicates were removed.
Supplemental material
Study selection criteria
We included randomised controlled trials (RCTs) where the population of interest was adults aged 18–65 years old without chronic disease; high adiposity or high body mass index (risk factors for chronic disease) were not exclusion criteria. We selected this study population because the relative homogeneity allows for comparing specific features and because youth, the elderly and those living with chronic diseases have different needs, barriers and enablers regarding physical activity that may not generalise to the general population. The intervention included a mobile app or an activity tracker enabling automated and continuous self-monitoring and feedback on physical activity measures. Our definition excludes pedometers and accelerometers if they did not offer ongoing access to tracked measures throughout time (either via the tracker’s display or by wirelessly syncing with an app). Given that this definition is compatible with the state-of-the-art in technologies to promote physical activity, we simply refer to them as ‘smartphone apps’ and ‘activity trackers’ throughout the paper.
The comparison group was either a true control (eg, given no intervention—usual care, waiting list—or an intervention not including an app or a tracker) or was an active control (ie, receiving a control intervention including an app or a tracker); and the main outcomes were measures of physical activity (online supplemental eTable 1 and eMethods 2).
Screening and data extraction
Title and abstract screening and full-paper screening were conducted by six pairs of independent investigators. Two investigators extracted information from the included studies into a Microsoft Excel spreadsheet (version 16.43): publication information, mobile technology, intervention characteristics, study duration, participant and setting characteristics, outcomes, behaviour change theories, retention rates (percentage completing follow-up assessment), engagement measures, funding sources, conflicts of interest, incentives for participation, adherence to reporting guidelines, personalisation and gamification features. Coding of BCTs according to the BCT taxonomy8 was conducted by three trained investigators. Included studies were assessed independently by two researchers using Cochrane’s risk of bias tool (domains assessed: random sequence allocation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data and selective reporting).32 33 Disagreements in screening, data extraction and risk of bias assessment were resolved by a third investigator. Data extraction and coding of BCTs were not conducted independently. For multiarm trials, data extraction was conducted for the two arms of interest (online supplemental eMethods 3). Data extraction was complemented with information from protocol papers, trial registrations and emails to authors, as well as known basic features of commercial trackers and mobile apps.
Strategy for data synthesis
A narrative synthesis was conducted for all studies. Studies for which it was possible to calculate an effect size were combined for a summary effect. Outcomes from cluster RCTs were included when adjusted for the effects of clustering. Whenever a single study reported multiple outcomes, the outcome to be included in the meta-analysis was selected through consensus among the authors following predefined rules to minimise bias (online supplemental eMethods 3).
Continuous outcomes were pooled together and all effect sizes were transformed into the standardised difference in means (SDM).34 Estimates of mean physical activity effect sizes were also converted from SDM to number of steps per day for ease of interpretation (online supplemental eMethods 4).
We used random effects models for all analyses; the between-studies variance (T 2) was estimated using the method of moments. We used I2 to describe the proportion of the variance in observed effects that is due to variance in true effects.35 The presence of publication bias was evaluated by the use of a funnel plot and the Duval and Tweedie trim-and-fill method.35 We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system for grading the body of evidence.36
Sensitivity analyses, subgroup analyses and metaregression
Seven sensitivity analyses were conducted to assess the robustness of the findings (online supplemental eMethods 5). The cause of observed statistical heterogeneity was explored using subgroup analysis. We conducted 27 subgroup analyses, of which 16 were planned and 11 were post hoc (online supplemental eMethods 6). We conducted metaregression with statistically significant moderators identified in subgroup analyses, a dichotomous variable representing studies where the app or tracker was the only difference between intervention and control, and continuous moderators (number of BCTs in the intervention, retention rate and study duration) for hypothesis-generating purposes. R2 was calculated to determine the proportion of total between-study variance explained by the model. Comprehensive Meta-Analysis V.3 was used for all computations. The significance level for all statistical tests was set at a p value of <0.05, two-tailed; 95% CIs were calculated where applicable.
Patient and public involvement
Although this study contained no direct consumer involvement, post hoc subgroup analyses were informed by previous work where consumer perspectives and needs in a physical activity intervention were explored.37 The results from the present study will be disseminated through the institutional websites and press releases.
Results
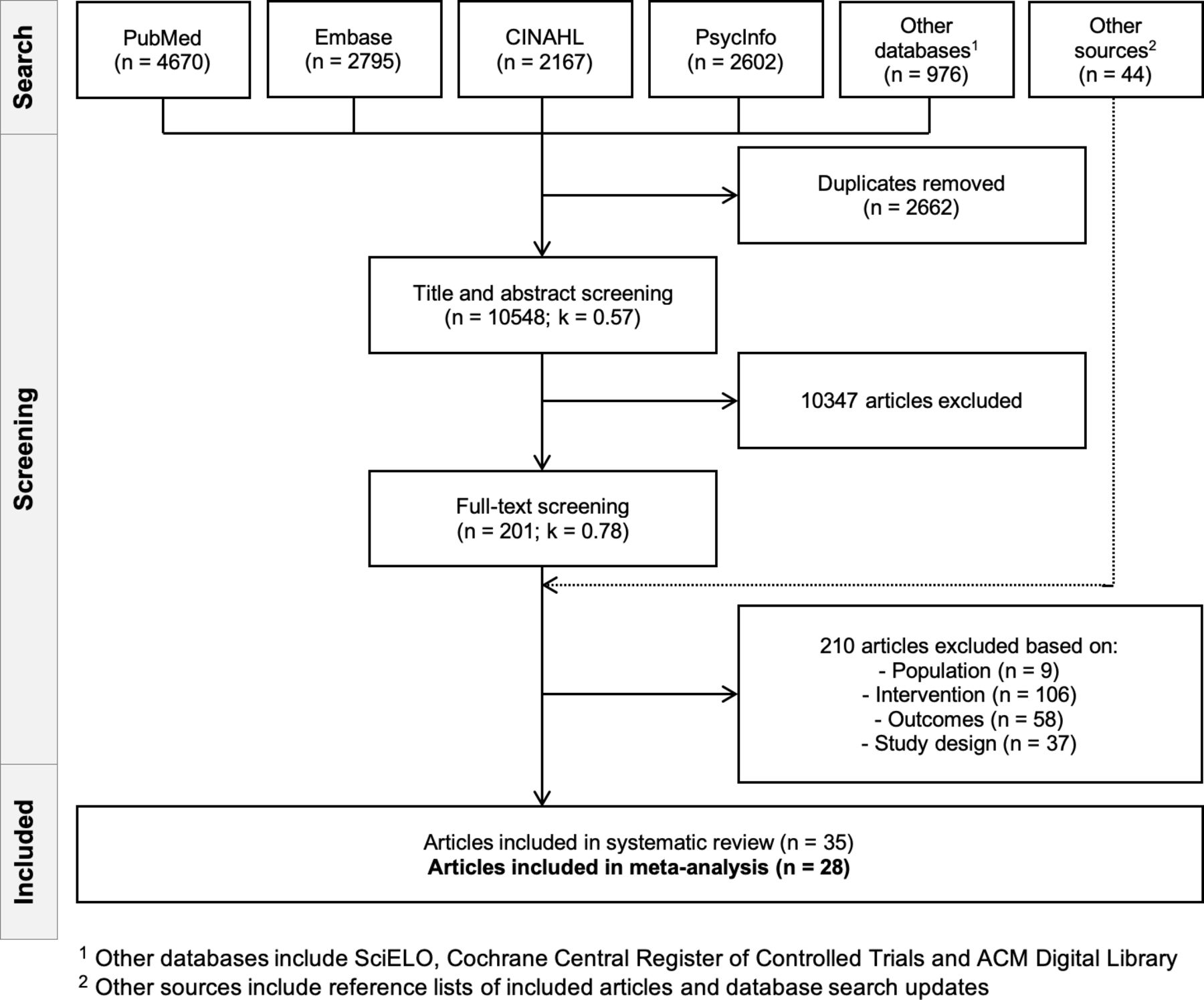
The database search retrieved 10 548 articles, after 2662 duplicates were removed (figure 1). After title and abstract screening, 10 347 articles were excluded. Full-text screening was conducted for the remaining 201 papers; 44 additional articles were found via updates of the database searches and reference lists of included papers. A further 210 articles were excluded (online supplemental eResults 1). The kappa statistic was 0.57 (fair agreement) for the title and abstract screening and 0.78 (substantial agreement) for the full-text screening, before consensus agreement was reached (online supplemental eTable 2). Although 35 studies met inclusion criteria, in 7 studies it was not possible to calculate an effect size to include in the meta-analysis (online supplemental eTables 3-5). The final number of included studies was 28.38–65 Of these, one was a doctoral thesis40 and another was a working paper57; the remaining were published articles.
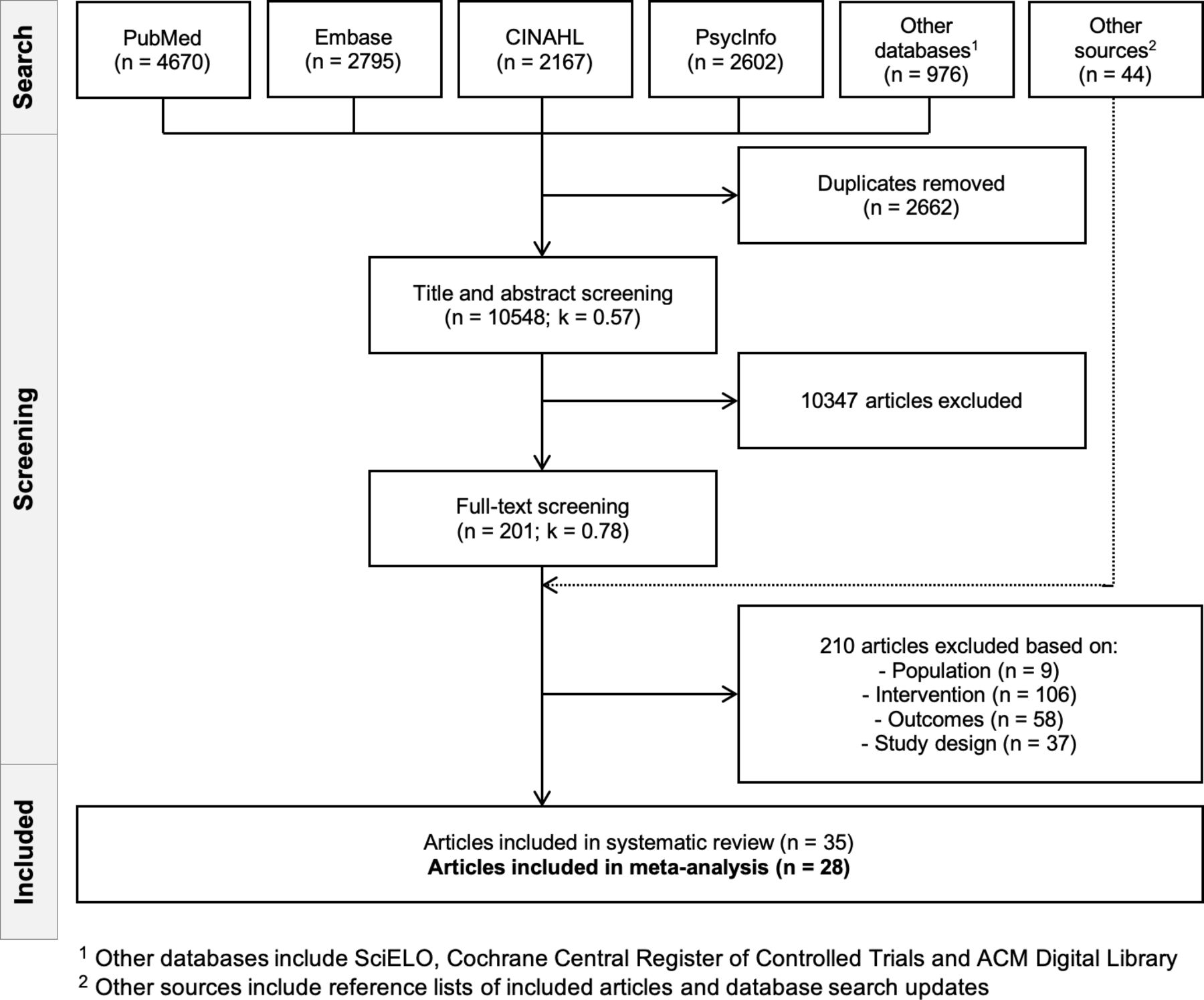
Flowchart of included studies. A total of 28 studies were included in the meta-analysis. 1Other databases include SciELO, Cochrane Central Register of Controlled Trials and ACM Digital Library. 2Other sources include reference lists of included articles and database search updates.
Description of included studies
The 28 studies were published between 2014 and 2019, and were mainly (n=20) conducted in the USA39 40 45 47–61 63 64 (table 1). Study duration varied between 2 and 40 weeks (mean duration: 13 weeks). Studies involved a total of 7454 participants, including 2107 (28%) women; 14 studies had a sample size smaller than 100, and 17 studies had less than 50 participants in the active intervention arm. In 12 studies, recruitment included only physically inactive or sedentary adults,40–42 46–48 51 54 55 57 58 64 and in 6 studies, recruitment included only overweight or obese individuals.38 41 47 50 53 64 Risk of bias was assessed as low for at least 4 out of 6 categories in 17 studies38 40 42–45 48–50 52 53 56 58 60 61 64 65 (online supplemental eTable 6). In seven articles, the authors declared relevant conflicts of interest38 45 48 50 53 56 60 (three papers had no conflict of interest statement, online supplemental eTable 7). Adherence to reporting guidelines was explicitly mentioned in eight studies40–43 48 49 58 65 (online supplemental eTable 7). Physical activity outcomes were measured with a research-grade accelerometer in 11 studies,38 40 42–44 46 47 51 55 59 64 self-reported (questionnaire) in 3 studies,39 41 63 and assessed with a mobile app or consumer-grade activity tracker in 14 studies45 48–50 52–54 56–58 60–62 65 (online supplemental eTable 8). Daily step count was the outcome in 21 studies38 40 42 43 45 46 48–54 56 57 59–62 64 65 and moderate-to-vigorous physical activity was the outcome in four studies44 47 55 58; three studies had different outcomes (all self-reported)—weekly days exercised, total physical activity (min/week) and metabolic equivalents per week (online supplemental eTable 8). All extracted outcomes are openly available online (https://osf.io/d3rnu/).
Characteristics of studies included in the meta-analysis
Participant engagement with the intervention was mentioned in 18 studies (online supplemental eTable 9). There was inconsistency in metrics reported. The most commonly reported measure across studies was the percentage of daily usage (six studies),41 42 45 47–49 which varied between 58.3% and 97.4% (mean 79.9, SD 14.5). Four studies reported on engagement changes throughout time, showing progressively lower engagement with the intervention.43 44 51 55 Retention rates varied between 61% and 100% for the intervention group (mean 90.5%, SD 10.2) (online supplemental eTable 9). In 15 studies, participants received incentives for study compliance and completion, most commonly gift vouchers38 40–42 44 45 47 50 52–54 56 58–60 (online supplemental eTable 10).
Intervention and control group components and BCTs
Studies were grouped according to whether or not the control group involved a smartphone app or tracker enabling automatic self-monitoring and feedback: true control (12 studies)38–49 or active control (16 studies)50–65 (table 2). Most interventions (n=20) included a physical activity tracker, with or without a mobile app38–49 51 52 54 56 57 59 64 (12 studies included a tracker with an app); eight interventions used a smartphone app without a tracker53 55 58 60–63 65 (table 2 and online supplemental eTable 11). Other common intervention components included email,39 43 45 48 49 53–57 59–61 63 human involvement (face-to-face or phone calls)38 42 43 46 47 49 51 55 62 64 65 and text messaging.45 48 53 55 56 60 61 64 65 There were only five studies where the only different components between intervention and control were the tracker or the smartphone app for self-monitoring and feedback on physical activity.40 41 43 58 59
Components and BCTs in intervention and control groups*†
Behaviour change theories were mentioned in 19 studies,38 40–42 44–48 50–52 54–58 62 63 the most common being social cognitive theory40–42 46 52 55 58 (online supplemental eTable 11). The mean number of BCTs present in interventions was 8.1 (SD 3.2) and in controls it was 2.9 (SD 2.3). Apart from BCTs in the ‘feedback and monitoring’ group, the most common groups of BCTs present in the intervention were ‘goals and planning’ and ‘reward and threat’ (figure 2 and online supplemental eTable 11), and the most frequent techniques were goal setting,38 39 41 42 44–48 50 51 54 55 60–65 prompts/cues,43 45 48–52 54 55 57–59 62–65 instruction on how to perform the behaviour38 40 42–44 46 48 51 54 55 58 62 63 65 and social support.38 41 42 44–46 51 52 58 Gamification or exergames were present in 14 studies38 39 44–46 49 50 53 55–58 60 63 (online supplemental eTable 12). Personalisation features were mentioned in 12 studies,38 41 42 44–49 54 55 58 most commonly in the form of personalised goal setting,38 42 45 47 58 feedback42 44 46 49 54 58 and content41 44 48 (online supplemental eTable 13).

Mapping of BCTs in intervention and control groups of included studies. The most common BCTs present in the intervention were from the ‘feedback and monitoring’ group (B2, 60 BCTs across all 30 studies), followed by ‘goals and planning’ (B1, 47 BCTs across 22 studies) and ‘reward and threat’ (B10, 25 BCTs in 11 studies). BCT, behaviour change technique.
Meta-analysis and metaregression
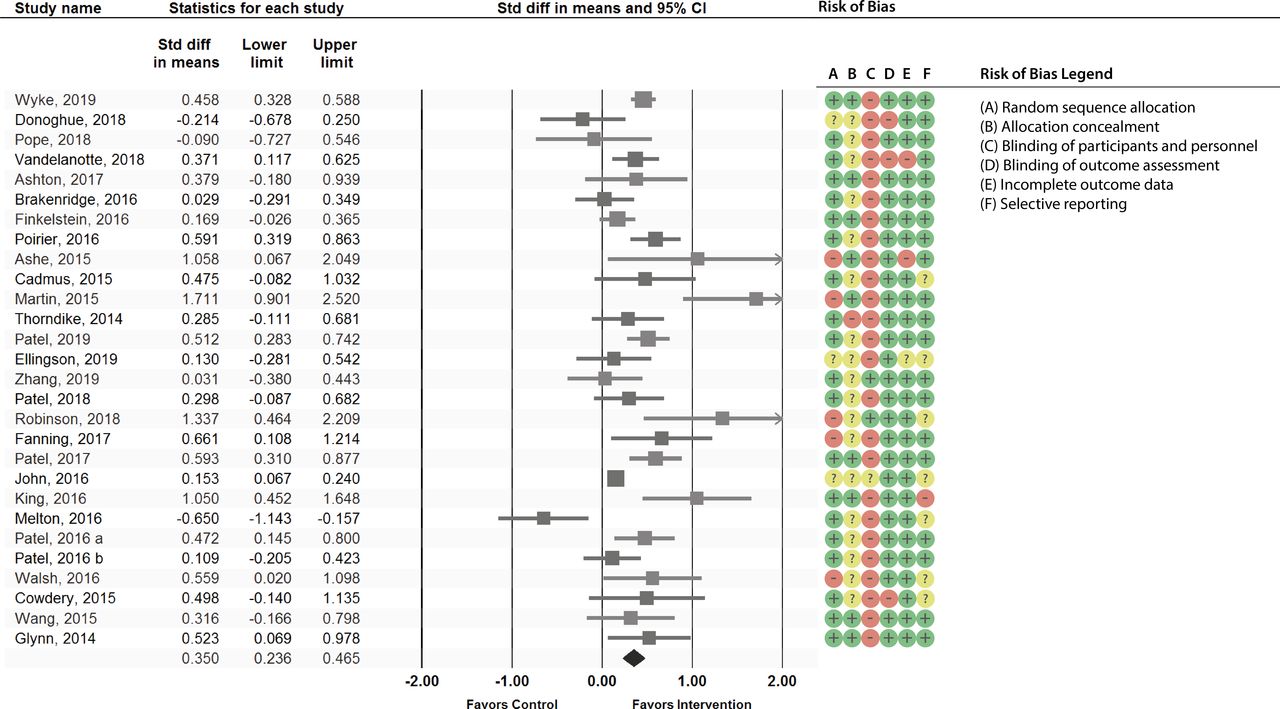
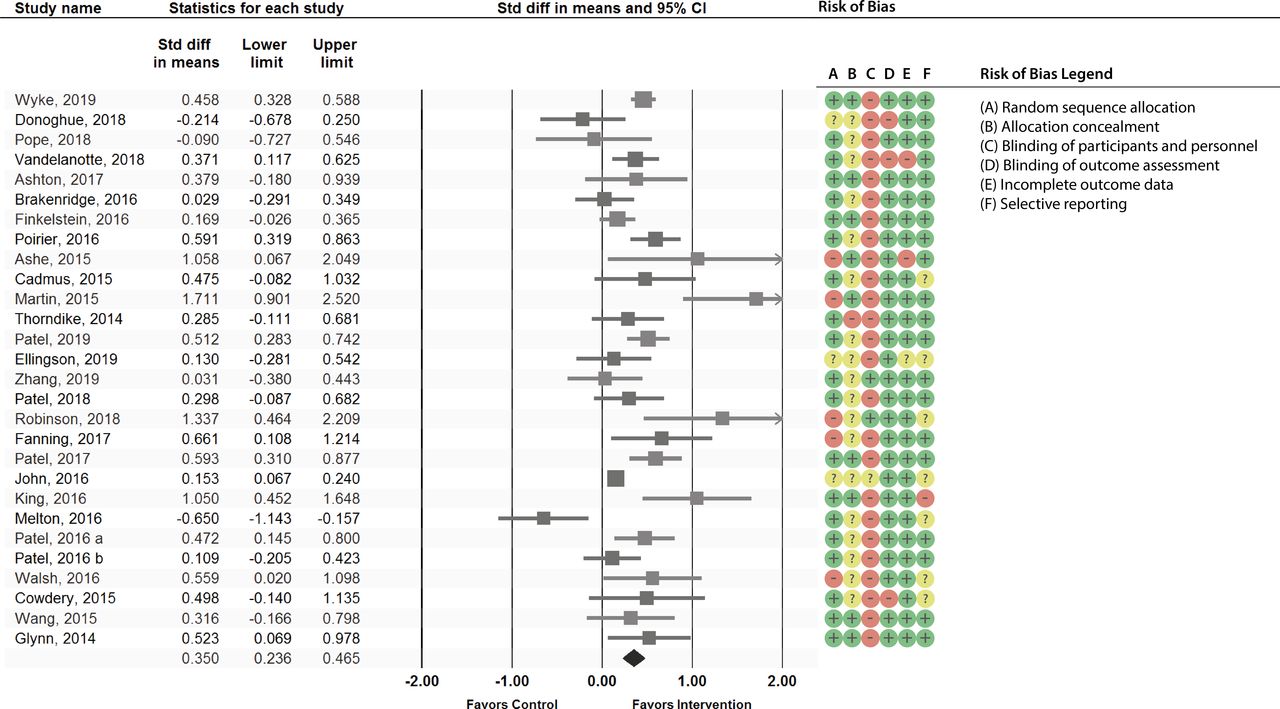
The meta-analysis showed a positive effect on physical activity favouring interventions, including smartphone apps or activity trackers versus true and active control (SDM 0.350, 95% CI 0.236 to 0.465, p<0.0001, I2=69%, T 2=0.051), corresponding to an increase of 1850 steps per day (95% CI 1247 to 2457) (figure 3). Despite signs of publication bias in the funnel plot, the Duval and Tweedie trim-and-fill method showed the adjusted estimate remained significant (online supplemental eFigure 1). We conducted seven sensitivity analyses and their results were consistent with the main analysis, showing a significant positive effect on physical activity favouring interventions including smartphone apps or activity trackers (online supplemental eTable 14). Grouping of studies by outcome type did, however, reveal a lower raw difference in means for daily step count (21 studies; 753.2, 95% CI 440.4 to 970.7). Forest plots of effect sizes ordered by retention rate, study duration and risk of bias are shown in online supplemental eFigures 2-4.
{kind=link}
{kind=link}
{kind=link}
Forest plot of effect sizes and 95% CIs representing the effect of interventions involving mobile applications or activity trackers in increasing physical activity (random effects model) with risk of bias assessment. The meta-analysis showed a positive effect on physical activity favouring interventions, including smartphone apps or activity trackers (SDM 0.350, 95% CI 0.236 to 0.465, p<0.0001, I2=69%, T 2=0.051), corresponding to an increase of 1850 steps per day (95% CI 1247 to 2457). Note: size of squares is proportional to study sample size. SDM, standardised difference in means.
Six of 27 subgroup analyses (3 out of 16 planned analyses) were statistically significant (online supplemental eFigures 5-10 and online supplemental eTable 15), namely, studies where the intervention had goals and planning (SDM 0.446, 95% CI 0.33 to 0.562, p<0.0001) or ‘graded tasks’ (SDM 0.512, 95% CI 0.337 to 0.687, p=0.031) BCTs, text messaging (SDM 0.495, 95% CI 0.335 to 0.654, p=0.028), personalisation (SDM 0.541, 95% CI 0.365 to 0.718, p=0.006), studies where the authors mentioned conflicts of interest (SDM 0.529, 95% CI 0.388 to 0.671, p=0.004) and studies mentioning behaviour change theories (SDM 0.449, 95% CI 0.312 to 0.587, p=0.018). Other subgroup analyses were not statistically significant, including analyses of studies where the intervention included an activity tracker or just an app, and studies where the tracker or the app were the only difference between intervention and control groups (online supplemental eTable 15). Heterogeneity was partially explained by differences in intervention components and populations: studies showing an I2 lower than 40% included those providing action planning or human contact, as well as studies not including activity trackers or focusing on overweight populations (online supplemental eTable 15).
A metaregression model including the moderators that showed significance in the previously mentioned subgroup analyses showed an adjusted R2 of 0.57 (table 3). A model including only the significant variables from the previous model, as well as two additional ones—retention rate in the intervention group and study duration—showed an adjusted R2 of 0.64, but study duration was not significant. A model replacing study duration with a dichotomous variable representing studies where the app or tracker were the only difference between intervention and control showed an adjusted R2 of 0.71, explaining 71% of the variance in effectiveness. Overall, text messaging, personalisation, and retention rate in the intervention were all significantly associated with intervention effectiveness, consistently across several models.
Metaregression
Discussion
Main findings
This is the first systematic review and meta-analysis of physical activity RCTs testing mobile apps or activity trackers that enable automated and continuous self-monitoring and feedback, in adults without chronic disease. Our findings suggest that interventions using apps or trackers have small-to-moderate effects on physical activity at a mean follow-up of 13 weeks, with an average increase of 1850 steps per day, compared with control. The available evidence is of low-to-moderate quality according to the GRADE system66 and should be interpreted within the context of existing heterogeneity and publication bias. However, adjusted results accounting for the presence of publication bias remained significant.
Interventions including text-messaging and personalisation features showed higher effectiveness, with moderate effect sizes. Some variables were significantly associated with higher effect sizes in subgroup analysis but not in the metaregression: interventions including BCTs from the goals and planning group or graded tasks, studies mentioning behaviour change theories and studies mentioning conflicts of interest. Retention rate in the intervention was significantly associated with intervention effectiveness. Engagement measures were seldom mentioned and varied between studies.
Comparison with existing literature
We found a significant improvement in physical activity with apps and trackers, consistent with several previous meta-analyses focusing on older mobile technologies.10 11 20 25 28 67–69 Our meta-analysis included a higher number of RCTs (28 vs an average of 17) and showed lower heterogeneity than other meta-analyses on mobile technologies (I2 of 69% vs an average of 75%).10 11 20 22 24–26 28 67–71 The lower heterogeneity may reflect the specificity of our inclusion criteria regarding population selection (adults without chronic disease) and the intervention (smartphone app or activity tracker enabling automated and continuous self-monitoring and feedback).
This study is consistent with previous work showing higher intervention effectiveness with the use of self-regulation techniques (self-monitoring, feedback and goal setting).9 11 72 Our review expands on this prior work by showing that automating self-monitoring and feedback does not seem to decrease intervention effectiveness, which could happen due to the lower effort and attention required from people to monitor their behaviour. In fact, lowering user burden may indeed contribute to higher engagement and effectiveness by decreasing the ‘costs’ of the intervention (such as the ‘opportunity costs’ of doing other valued activities).73 Self-regulation techniques are recognisably important in promoting physical activity,9 11 72 and self-regulation is a crucial concept in social cognitive theory, the most commonly mentioned theory in our study and related reviews.24 The higher prevalence of social cognitive theory and self-regulation techniques in our review may also explain our finding that interventions mentioning (ie, being based on) behaviour change theories were more effective, with previous meta-analyses suggesting that effectiveness may be more influenced by the specific BCTs used in an intervention than merely by the stated use of theory.74
As in other reviews, we found higher effectiveness of interventions including text messaging,75 suggesting that this long-standing delivery mode continues to play an important role in behavioural informatics. Text messaging allows the delivery of prompts and cues, a BCT associated with behaviour maintenance.76 Future research should explore whether the effect of text messages can be explained by their higher intrusiveness when compared with smartphone notifications (which can be switched off more easily). Additional studies with a longer duration should also explore the role of different components and BCTs in promoting engagement77 and intervention effectiveness in the long term.
Our study showed a higher average retention rate than the only other meta-analysis reporting this measure (90.5% vs 80%).11 In our analysis, retention was associated with effectiveness, whereas study duration was not. Furthermore, four studies reported on engagement changes over time, showing progressively lower usage43 44 51 55 despite their short duration—a phenomenon known as the law of attrition of health informatics interventions.78 Only one of these studies found a statistically significant improvement in physical activity at the end of the intervention,55 which suggests the importance of continued engagement for effectiveness. It thus remains unclear what the right ‘dose’ of app or tracker usage may be, or how it might vary for different people and circumstances. Future studies should consistently report engagement measures to allow future evaluation of the dose–response relationship between app or tracker usage and effectiveness.
Personalisation seems promising in promoting effective engagement with behaviour change interventions.73 79 80 Previous reviews of computer-tailored interventions to promote behaviour change have found higher effectiveness of interventions providing tailored content, that is, selecting communication content using data-driven decision rules.81 Recent developments in artificial intelligence may help leverage the richness of data routinely collected by smartphones and build machine learning models that optimise intervention content, timing and delivery, based on users’ preferences, behavioural patterns, and other individual and contextual data.82–84 In the future, mobile physical activity interventions may be able to deliver a core set of universally effective BCTs (eg, self-regulation), with additional techniques and features being personalised. Future research should explore users’ perspectives on personalisation and the potential downsides resulting from sharing large volumes of personal data for that purpose.
Strengths and limitations
Our study has several strengths. Our search strategy included peer-reviewed and grey literature. There was substantial agreement in full-text screening. Given that data extraction was hampered by incomplete intervention descriptions, with most studies not adhering to reporting guidelines, we complemented data extraction with information from protocol papers, registrations and emails to authors, as well as known basic features of commercial trackers and mobile apps. Data extraction was extensive and included coding of BCTs by three trained investigators, following the BCT taxonomy.8 Several sensitivity analyses were consistent with our main results. Our reporting of retention and engagement metrics and our analysis of the effectiveness of different features within the interventions are the most comprehensive to date.
Our review also has some limitations: (1) the search strategy was not peer reviewed; (2) data extraction and coding were not conducted independently and we could not measure intercoder agreement; (3) our coding of personalisation features was based on authors’ mention of this term or synonyms; (4) subgroup analyses and meta-regression should be interpreted as exploratory findings due to the possibility of mass significance and uncontrolled confounding; (5) there was considerable heterogeneity, which was partially explained by differences in intervention components and population; (6) there were changes from the protocol, which are acknowledged in the methods and supplements; (7) generalisation of our results to the female population is limited, given that only 28% of participants were women (due to the inclusion of a few large-scale studies targeting only men).
Implications
Interventions using smartphone apps or activity trackers seem promising from a clinical and public health perspective, promoting a significant step count increase of 1850 steps/day. These results are of public health importance according to recent evidence showing that any physical activity, regardless of intensity, is associated with lower mortality risk in a dose–response manner85 and that an increase of 1700 steps/day is significantly associated with lower mortality rates.86
Apps and trackers are becoming ubiquitous in people’s daily lives, with smartphone ownership surpassing three-quarters of the population and activity trackers being used by one-third of adults in the USA and UK.87 88 Despite growing access to these technologies, it is important to ensure that the needs of diverse groups are being met by closing the digital divide, promoting digital health literacy and fostering inclusive design strategies.89 Wide reach to different population groups is key to guaranteeing that improvements in physical activity from these interventions generate large effects at the population level, without worsening health inequities.
Enhancing the value of these interventions to consumers may boost long-term engagement and effectiveness, further increasing their impact. Promoting engagement beyond the initial ‘novelty phase’ is dependent on user experience, overall utility, and the ability to integrate with other devices and services.14 Integrating sensor data from apps and trackers with electronic health record data are also likely to be useful for patients and clinicians. This is now possible with the Apple Health app, which is able to pull in health data from healthcare institutions,12 operating as a personal health record. Such innovations, adding value to consumers, have the potential to spark a new generation of precision public health interventions.
The prescription of smartphone apps or activity trackers by clinicians to promote physical activity may extend the benefits of these interventions beyond the ‘worried well’ early adopters.90 91 Primary care behaviour counselling interventions to promote physical activity are known to consistently improve important intermediate health outcomes, with evidence of a dose–response.92 Given increasing time constraints in clinical practice, a brief intervention during the consultation may consist of prescribing an app or tracker, as part of a shared decision-making process, to individuals who seem ready to make behavioural changes.
Conclusion
We performed a systematic review and meta-analysis of RCTs and found that interventions using smartphone apps or physical activity trackers have a significant small-to-moderate effect in increasing physical activity (1850 steps daily). These interventions were more effective when including text-messaging or personalisation features. Given the wide and increasing reach of smartphones, even modest improvements in physical activity can produce large effects at the population level. Longer-duration studies with more diverse populations should explore long-term effectiveness and sustained engagement.
What is already known
Waist-worn pedometers can increase physical activity in the short term but are burdensome to use. Reviews of apps and trackers have shown inconsistent results, with high heterogeneity. Existing reviews of apps and trackers have not yet focused on healthy adults and on state-of-the-art technology, enabling automated and continuous self-monitoring and feedback.
What are the new findings
Interventions using contemporary mobile apps or physical activity trackers are effective in promoting physical activity, with a statistically significant effect size of public health relevance. These interventions were more effective when including text-messaging or personalisation features. These results are valuable to clinicians, who may prescribe apps and trackers as part of a shared decision-making process to individuals who seem ready to make behavioural changes.
Acknowledgments
We thank Annie Y S Lau, Monique Lepouris and Keyu Wang for help with title and abstract screening.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @LilianaLaranjo, @DrMelodyDing
DD and BH contributed equally.
Contributors The corresponding author (LL) attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. LL is the guarantor. Conception and design of the work: LL; database searching: LL, BC, MLA; title, abstract and full-text screening: LL, BC, BH, DR, ALN, EG, HLT, MLA; outcome data extraction: LL, BH; BCT coding: LL, EG, HLT; risk of bias: LL, BH, ALN; figure 1: BC, LL; figures 2 and 3: BK, LL; data analysis and interpretation: LL, BH, DD, DWB, JCQ, EC, DR, HLT, KPD, GCN; first draft: LL; critical revision of drafts for important intellectual content: LL, DD, DWB, BH, BK, JCQ, HLT, KPD, DR, EG, ALN, GCN MLA, BC, EC; final approval of the version to be published: LL, DD, DWB, BH, BK, JCQ, HLT, KPD, DR, EG, ALN, GCN, MLA, BC, EC.
Funding This research was supported by the National Health and Medical Research Council (grant APP1134919, Centre for Research Excellence in Digital Health). The funder had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The study-specific summary data included in the meta-analysis can be obtained from the corresponding author (liliana.laranjo@mq.edu.au).
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.