Black outpatients are less likely to receive buprenorphine than White outpatients
Opioid mortality rates remain at record highs in the United States. Buprenorphine is an effective, first-line treatment for opioid use disorder. This study tested whether, despite a substantial increase in access to this life-saving medication overall, racial/ethnic minorities may not have equal access.
While methadone is an effective, low costmedication for opioid use disorder that’s easily accessible in theUnited States through community clinics, a newer medication for opioid use disorder, buprenorphine, is more effective for some people. Buprenorphine also allows for more freedom and flexibility given that this medication is picked up at the pharmacy and taken home, while methadone patients must get this medication from opioid treatment programs and, at least initially, attend the programs daily. Buprenorphine, however,is relatively expensive, and can only be prescribed by physicians or nurse practitioners with a special license. It is thought that wealthier, White individuals with more financial and healthcare resources(e.g., health insurance) have better access to this buprenorphine, while racial/ethnic minorities who tend to be less wealthy, on average, may have difficulty accessingthis medication.This studyexplored this hypothesis.
HOW WAS THIS STUDY CONDUCTED?
The research teamcombined data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey outpatient department component from 2004 to 2015. The surveys, which provide nationally–representative estimates of outpatient care provided in the United States by non–federally–employed physicians, capture physician-reported medications prescribed during each office visit as well as demographic characteristics and expected source of payment. Notably, results reflect buprenorphine prescriptions for all individuals, not necessarily just people with opioid use disorder. The sample was approximately 88% White, 8% Black, 4% Other, and 51% female.
WHAT DID THIS STUDY FIND?
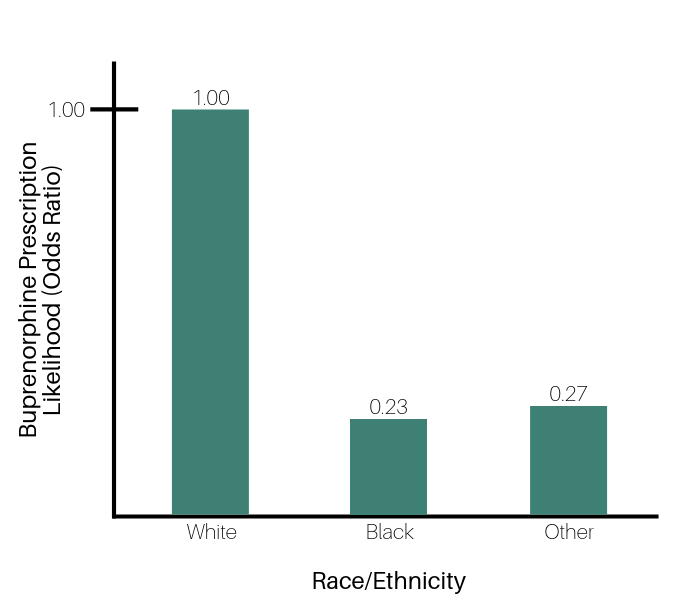
From 2004 to 2015, the number of prescriber visits for buprenorphinerose from 0.04% to 0.36% of all outpatient prescriber visits, representing 13.4 million visits between 2012 and 2015.After accounting for payment method, sex, and age, the study’s authors found that White patients were 0.77 times more likely to receive buprenorphine at their prescriber visits than their Black counterparts.
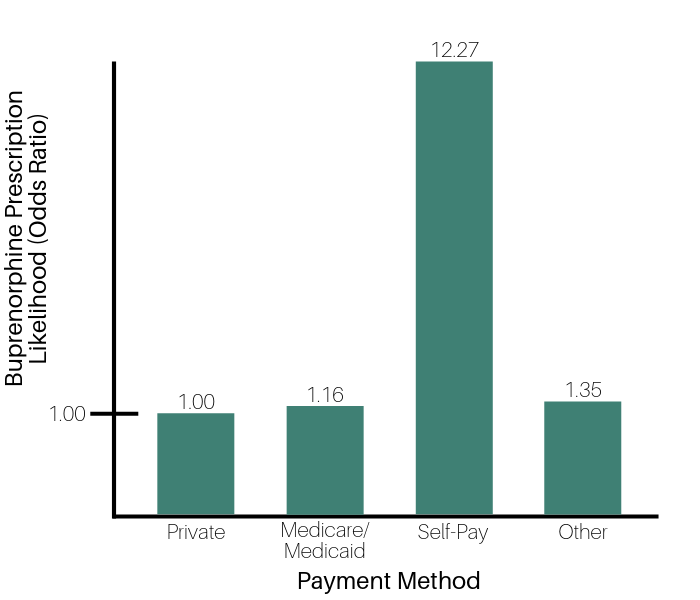
Results also show that across all time periods assessed,self-pay patients – in other words, those with more financialresources – were 12.3 times more likely to be prescribed buprenorphine compared to those with private insurance. There was also a marked increase in the number of individuals receiving buprenorphine via self-pay from 2008-2015.
Figure 1. Odds ratios depicting likelihood of buprenorphine prescriptions, where White individuals act as the comparison group, demonstrating that individuals identifying as Black and Other are significantly less likely to be prescribed buprenorphine than those identifying as White.
Figure 2. Odds ratios depicting likelihood of a buprenorphine prescription being given based on an individual’s payment method for their medical treatment, where private pay acts as the comparison group, indicating that self-pay patients are significantly more likely to receive a buprenorphine prescription as compared to all other payment methods.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The authors’ findings confirm what has long been suspected by addiction treatment experts, that White individuals and those with greater financial/healthcare resources are more likely to receive buprenorphine tomanage opioid use disorder, versus racial/ethnic minorities and those with lessfinancial/healthcare resources. This is in spite of the fact that opioid use disorder occurs at similar rates across racial groups and socioeconomic classes. Further, given this study was agnostic to whether individuals had opioid use disorder, there is no compelling reason why prescription rates should be different by race.This finding is consistent with previous work by Stein and colleagues and Hansen and colleagues, showing racial inequities in access to buprenorphine. Findings also highlight a possible trend in providers licensed to prescribe buprenorphine taking cash only, meaning buprenorphine may be becoming even less accessible to those without financial means.
These findings provide a snapshot of buprenorphine prescription in the United States from 2004–2015, and therefore can’t speak to buprenorphine prescription patterns since 2015.
There are numerous other social factors that may be influencing buprenorphine prescription in the United States that the authors were not able to account for. For instance, this study was unable to determine whether any differences in beliefs or attitudes toward medication use may differ across different racial/ethnic groups.
BOTTOM LINE
For individuals and families seeking recovery: Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with greater financial/healthcare resources. For many, accessing buprenorphine can be challenging, but it is worth the extra effort, especially for those for whom methadone has not proven effective. Call your insurance provider if you have one for referrals to buprenorphine–licensed providers in your area. You can also accessSAMHSA’s buprenorphine practitioner locatorto find providers who can prescribe this medication.
For treatment professionals and treatment systems: Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with financial/healthcare resources.Greater understanding as to why individuals from racial/ethnic minorities are not accessing these medications as frequently as White individualsis important to understand. Professionals might need to inquire more explicitly among minority populations whether there are belief, attitude, economic/financial, or other logistical barriers preventing use of these life-saving medications. Eligible prescribers such as medical doctors and nurse practitioners should get licensed to provide buprenorphine.
For scientists:Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with financial/healthcare resources.Greater understanding as to why individuals from racial/ethnic minorities are not accessing these medications as frequently as White individuals is important to understand. Professionals might need to inquire more explicitly among minority populations whether there are belief, attitude, economic, or other logistical barriers preventing use of these life-saving medications. More work is needed to further parse out these disparities so that this research may inform policy changes to improve access to this medication. For instance, work is needed describing in which parts of the United States buprenorphine is most available and most prescribed.
For policy makers: Buprenorphine is a life-saving opioid use disorder medication, but the reviewed findings indicate that racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with greater financial/healthcare resources. Policies are desperately needed that increase access to this medication. One simple way to do this could be to ease restriction on prescribing privileges so physicians do not require a special license to prescribe this medication.Supporting efforts to eliminate the need for a special license to prescribe buprenorphine could help accomplish this. To this point, increasing limits on the number of individuals to whom a prescriber can prescribe buprenorphine has been shown tolead to large increases in buprenorphine availability.
While methadone is an effective, low costmedication for opioid use disorder that’s easily accessible in theUnited States through community clinics, a newer medication for opioid use disorder, buprenorphine, is more effective for some people. Buprenorphine also allows for more freedom and flexibility given that this medication is picked up at the pharmacy and taken home, while methadone patients must get this medication from opioid treatment programs and, at least initially, attend the programs daily. Buprenorphine, however,is relatively expensive, and can only be prescribed by physicians or nurse practitioners with a special license. It is thought that wealthier, White individuals with more financial and healthcare resources(e.g., health insurance) have better access to this buprenorphine, while racial/ethnic minorities who tend to be less wealthy, on average, may have difficulty accessingthis medication.This studyexplored this hypothesis.
HOW WAS THIS STUDY CONDUCTED?
The research teamcombined data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey outpatient department component from 2004 to 2015. The surveys, which provide nationally–representative estimates of outpatient care provided in the United States by non–federally–employed physicians, capture physician-reported medications prescribed during each office visit as well as demographic characteristics and expected source of payment. Notably, results reflect buprenorphine prescriptions for all individuals, not necessarily just people with opioid use disorder. The sample was approximately 88% White, 8% Black, 4% Other, and 51% female.
WHAT DID THIS STUDY FIND?
From 2004 to 2015, the number of prescriber visits for buprenorphinerose from 0.04% to 0.36% of all outpatient prescriber visits, representing 13.4 million visits between 2012 and 2015.After accounting for payment method, sex, and age, the study’s authors found that White patients were 0.77 times more likely to receive buprenorphine at their prescriber visits than their Black counterparts.
Results also show that across all time periods assessed,self-pay patients – in other words, those with more financialresources – were 12.3 times more likely to be prescribed buprenorphine compared to those with private insurance. There was also a marked increase in the number of individuals receiving buprenorphine via self-pay from 2008-2015.
Figure 1. Odds ratios depicting likelihood of buprenorphine prescriptions, where White individuals act as the comparison group, demonstrating that individuals identifying as Black and Other are significantly less likely to be prescribed buprenorphine than those identifying as White.
Figure 2. Odds ratios depicting likelihood of a buprenorphine prescription being given based on an individual’s payment method for their medical treatment, where private pay acts as the comparison group, indicating that self-pay patients are significantly more likely to receive a buprenorphine prescription as compared to all other payment methods.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The authors’ findings confirm what has long been suspected by addiction treatment experts, that White individuals and those with greater financial/healthcare resources are more likely to receive buprenorphine tomanage opioid use disorder, versus racial/ethnic minorities and those with lessfinancial/healthcare resources. This is in spite of the fact that opioid use disorder occurs at similar rates across racial groups and socioeconomic classes. Further, given this study was agnostic to whether individuals had opioid use disorder, there is no compelling reason why prescription rates should be different by race.This finding is consistent with previous work by Stein and colleagues and Hansen and colleagues, showing racial inequities in access to buprenorphine. Findings also highlight a possible trend in providers licensed to prescribe buprenorphine taking cash only, meaning buprenorphine may be becoming even less accessible to those without financial means.
These findings provide a snapshot of buprenorphine prescription in the United States from 2004–2015, and therefore can’t speak to buprenorphine prescription patterns since 2015.
There are numerous other social factors that may be influencing buprenorphine prescription in the United States that the authors were not able to account for. For instance, this study was unable to determine whether any differences in beliefs or attitudes toward medication use may differ across different racial/ethnic groups.
BOTTOM LINE
For individuals and families seeking recovery: Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with greater financial/healthcare resources. For many, accessing buprenorphine can be challenging, but it is worth the extra effort, especially for those for whom methadone has not proven effective. Call your insurance provider if you have one for referrals to buprenorphine–licensed providers in your area. You can also accessSAMHSA’s buprenorphine practitioner locatorto find providers who can prescribe this medication.
For treatment professionals and treatment systems: Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with financial/healthcare resources.Greater understanding as to why individuals from racial/ethnic minorities are not accessing these medications as frequently as White individualsis important to understand. Professionals might need to inquire more explicitly among minority populations whether there are belief, attitude, economic/financial, or other logistical barriers preventing use of these life-saving medications. Eligible prescribers such as medical doctors and nurse practitioners should get licensed to provide buprenorphine.
For scientists:Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with financial/healthcare resources.Greater understanding as to why individuals from racial/ethnic minorities are not accessing these medications as frequently as White individuals is important to understand. Professionals might need to inquire more explicitly among minority populations whether there are belief, attitude, economic, or other logistical barriers preventing use of these life-saving medications. More work is needed to further parse out these disparities so that this research may inform policy changes to improve access to this medication. For instance, work is needed describing in which parts of the United States buprenorphine is most available and most prescribed.
For policy makers: Buprenorphine is a life-saving opioid use disorder medication, but the reviewed findings indicate that racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with greater financial/healthcare resources. Policies are desperately needed that increase access to this medication. One simple way to do this could be to ease restriction on prescribing privileges so physicians do not require a special license to prescribe this medication.Supporting efforts to eliminate the need for a special license to prescribe buprenorphine could help accomplish this. To this point, increasing limits on the number of individuals to whom a prescriber can prescribe buprenorphine has been shown tolead to large increases in buprenorphine availability.
While methadone is an effective, low costmedication for opioid use disorder that’s easily accessible in theUnited States through community clinics, a newer medication for opioid use disorder, buprenorphine, is more effective for some people. Buprenorphine also allows for more freedom and flexibility given that this medication is picked up at the pharmacy and taken home, while methadone patients must get this medication from opioid treatment programs and, at least initially, attend the programs daily. Buprenorphine, however,is relatively expensive, and can only be prescribed by physicians or nurse practitioners with a special license. It is thought that wealthier, White individuals with more financial and healthcare resources(e.g., health insurance) have better access to this buprenorphine, while racial/ethnic minorities who tend to be less wealthy, on average, may have difficulty accessingthis medication.This studyexplored this hypothesis.
HOW WAS THIS STUDY CONDUCTED?
The research teamcombined data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey outpatient department component from 2004 to 2015. The surveys, which provide nationally–representative estimates of outpatient care provided in the United States by non–federally–employed physicians, capture physician-reported medications prescribed during each office visit as well as demographic characteristics and expected source of payment. Notably, results reflect buprenorphine prescriptions for all individuals, not necessarily just people with opioid use disorder. The sample was approximately 88% White, 8% Black, 4% Other, and 51% female.
WHAT DID THIS STUDY FIND?
From 2004 to 2015, the number of prescriber visits for buprenorphinerose from 0.04% to 0.36% of all outpatient prescriber visits, representing 13.4 million visits between 2012 and 2015.After accounting for payment method, sex, and age, the study’s authors found that White patients were 0.77 times more likely to receive buprenorphine at their prescriber visits than their Black counterparts.
Results also show that across all time periods assessed,self-pay patients – in other words, those with more financialresources – were 12.3 times more likely to be prescribed buprenorphine compared to those with private insurance. There was also a marked increase in the number of individuals receiving buprenorphine via self-pay from 2008-2015.
Figure 1. Odds ratios depicting likelihood of buprenorphine prescriptions, where White individuals act as the comparison group, demonstrating that individuals identifying as Black and Other are significantly less likely to be prescribed buprenorphine than those identifying as White.
Figure 2. Odds ratios depicting likelihood of a buprenorphine prescription being given based on an individual’s payment method for their medical treatment, where private pay acts as the comparison group, indicating that self-pay patients are significantly more likely to receive a buprenorphine prescription as compared to all other payment methods.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The authors’ findings confirm what has long been suspected by addiction treatment experts, that White individuals and those with greater financial/healthcare resources are more likely to receive buprenorphine tomanage opioid use disorder, versus racial/ethnic minorities and those with lessfinancial/healthcare resources. This is in spite of the fact that opioid use disorder occurs at similar rates across racial groups and socioeconomic classes. Further, given this study was agnostic to whether individuals had opioid use disorder, there is no compelling reason why prescription rates should be different by race.This finding is consistent with previous work by Stein and colleagues and Hansen and colleagues, showing racial inequities in access to buprenorphine. Findings also highlight a possible trend in providers licensed to prescribe buprenorphine taking cash only, meaning buprenorphine may be becoming even less accessible to those without financial means.
These findings provide a snapshot of buprenorphine prescription in the United States from 2004–2015, and therefore can’t speak to buprenorphine prescription patterns since 2015.
There are numerous other social factors that may be influencing buprenorphine prescription in the United States that the authors were not able to account for. For instance, this study was unable to determine whether any differences in beliefs or attitudes toward medication use may differ across different racial/ethnic groups.
BOTTOM LINE
For individuals and families seeking recovery: Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with greater financial/healthcare resources. For many, accessing buprenorphine can be challenging, but it is worth the extra effort, especially for those for whom methadone has not proven effective. Call your insurance provider if you have one for referrals to buprenorphine–licensed providers in your area. You can also accessSAMHSA’s buprenorphine practitioner locatorto find providers who can prescribe this medication.
For treatment professionals and treatment systems: Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with financial/healthcare resources.Greater understanding as to why individuals from racial/ethnic minorities are not accessing these medications as frequently as White individualsis important to understand. Professionals might need to inquire more explicitly among minority populations whether there are belief, attitude, economic/financial, or other logistical barriers preventing use of these life-saving medications. Eligible prescribers such as medical doctors and nurse practitioners should get licensed to provide buprenorphine.
For scientists:Buprenorphine is an effective, first-line opioid use disorder medication, but the reviewed findings indicate racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with financial/healthcare resources.Greater understanding as to why individuals from racial/ethnic minorities are not accessing these medications as frequently as White individuals is important to understand. Professionals might need to inquire more explicitly among minority populations whether there are belief, attitude, economic, or other logistical barriers preventing use of these life-saving medications. More work is needed to further parse out these disparities so that this research may inform policy changes to improve access to this medication. For instance, work is needed describing in which parts of the United States buprenorphine is most available and most prescribed.
For policy makers: Buprenorphine is a life-saving opioid use disorder medication, but the reviewed findings indicate that racial/ethnic minorities and those without financial means are not able to access it in the same way as White individuals and those with greater financial/healthcare resources. Policies are desperately needed that increase access to this medication. One simple way to do this could be to ease restriction on prescribing privileges so physicians do not require a special license to prescribe this medication.Supporting efforts to eliminate the need for a special license to prescribe buprenorphine could help accomplish this. To this point, increasing limits on the number of individuals to whom a prescriber can prescribe buprenorphine has been shown tolead to large increases in buprenorphine availability.